Much of the recent criticism aimed at Don Berwick, the new CMS Administrator, is, in my opinion, unfair and politically motivated. Other criticism is legitimate, as some in the quality and infection prevention communities have disagreed with his willingness to vigorously pursue some strategies that lack strong evidence. This was discussed in a blog posting a few months ago by Bob Wachter. Now there's a new issue emerging. Sen. Chuck Grassley has requested that Berwick disclose the funding of the non-profit he founded, the Institute for Healthcare Improvement. According to IHI's 2008 form 990, which can be viewed at the Guidestar website, Berwick's reportable compensation was $2.3 million in 2008. Regardless of the motivation behind Grassley's information request, whether Berwick has conflicts of interest is a legitimate question.
Addendum (8/1/10, 9:50 AM): Click here for more.
Saturday, July 31, 2010
Thursday, July 29, 2010
CDC's recommendations for flu vaccine
CDC has just released its annual recommendations for influenza vaccination for the upcoming flu season. You can view the document here. There are very few new recommendations. The biggest change is that vaccination is now recommended for all persons 6 months of age and older. The publication notes the availability of high dose vaccine for persons 65 years and over but offers no recommendations regarding its use.
Wednesday, July 28, 2010
My surgeon has S. aureus!
 Don't panic! Just based on probability a surgeon would have a 30% chance of being colonized with MSSA and perhaps a 1% chance of being colonized with MRSA. Researchers at NYU Hospital for Joint Diseases recently screened a total of 135 orthopedic surgeons for MRSA and MSSA nasal colonization. In the 74 attendings, 2.7% were MRSA+ and 23.3% were MSSA+. The story was a bit more interesting in the 61 residents with 59% MSSA+ and none MRSA colonized. Overall, 36% were MSSA+ and 1.5% were MRSA+, which is about what we would have guessed before the study.
Don't panic! Just based on probability a surgeon would have a 30% chance of being colonized with MSSA and perhaps a 1% chance of being colonized with MRSA. Researchers at NYU Hospital for Joint Diseases recently screened a total of 135 orthopedic surgeons for MRSA and MSSA nasal colonization. In the 74 attendings, 2.7% were MRSA+ and 23.3% were MSSA+. The story was a bit more interesting in the 61 residents with 59% MSSA+ and none MRSA colonized. Overall, 36% were MSSA+ and 1.5% were MRSA+, which is about what we would have guessed before the study.These results are similar to Cecilia Johnston's report of healthcare worker colonization at Johns Hopkins a few years ago. She reported 28% S. aureus colonization (95% confidence interval [CI], 22%‐34%) and 2% MRSA colonization (95% CI, 0.04%‐4.0%). I pasted in Cecilia's results to highlight the fact that she calculated confidence intervals for each proportion. The NYU researchers were surprised by the high proportion of residents with MSSA colonization. Sure, the level was high, but if they would have calculated the 95% CI, which was 46%-71%, they might have been less excited.
It's possible that the long hours spent in direct patient care might be risk factors for MSSA colonization, as would frequently performing dressing changes, but these would not be unique to ortho residents. Perhaps they should repeat the study in the same residents at a later point to determine what proportion is transient vs persistent colonization. Of course, it would be nice to repeat the study in other cohorts of ortho residents and ortho nurses.
They also reported that patients screened prior to THR, TKR and major spine surgery at their hospital had 2% MRSA and only 18% MSSA colonization. It would have been nice to read more information about these patients, such as recent antibiotic exposure.
Schwarzkopf et al. in Journal of Bone and Joint Surgery (America): PubMed or JBJS
Johnston et al. in December 2007 ICHE
Easy confidence interval for proportion calculator: link
Tuesday, July 27, 2010
Is PJP a nosocomial infection?
There's a paper in the August 1 issue of Clinical Infectious Diseases of interest to the infection prevention community. In this French study, investigators sought to determine whether Pneumocystis jirovecii could be detected in the air near 19 patients who had documented infection with the organism. The proportion of samples yielding Pneumocystis significantly decreased with distance from the patient. Of samples obtained 1 m from the patient, 79% were positive; 69% were positive at a distance of 3 m from the patient; 42% at 5 m (at the entrance to the patient room); and 33% were positive at 8 m (in the corridor outside the patient room). The authors note that existing animal models have documented host-to-host transmission.
So the real question is whether current infection control guidelines are robust enough. CDC recommends not placing another immunocompromised patient in the same room as a patient with PJP (p. 108 of this document). Most HIV patients with PJP are initially placed in airborne precautions to rule out concomitant infection with M. tuberculosis. Tuberculosis can be ruled out in 1-2 days, and fortunately there were no positive samples at 5 or 8 m >1 day after the start of treatment for PCP.
My bigger concern is for transplant patients, who in many hospitals are geographically concentrated on specific units. Often these patients are able to ambulate in hallways, where they could encounter the organism outside an infected patient's room. Moreover, rooms in bone marrow transplant units are often at positive pressure, which would likely drive more organisms outside the room. I guess the good news is that we don't see many transplant patients with PJP since many receive prophylaxis for a period of time post-transplant, but it's probably an issue that we need to monitor a little more closely.
So the real question is whether current infection control guidelines are robust enough. CDC recommends not placing another immunocompromised patient in the same room as a patient with PJP (p. 108 of this document). Most HIV patients with PJP are initially placed in airborne precautions to rule out concomitant infection with M. tuberculosis. Tuberculosis can be ruled out in 1-2 days, and fortunately there were no positive samples at 5 or 8 m >1 day after the start of treatment for PCP.
My bigger concern is for transplant patients, who in many hospitals are geographically concentrated on specific units. Often these patients are able to ambulate in hallways, where they could encounter the organism outside an infected patient's room. Moreover, rooms in bone marrow transplant units are often at positive pressure, which would likely drive more organisms outside the room. I guess the good news is that we don't see many transplant patients with PJP since many receive prophylaxis for a period of time post-transplant, but it's probably an issue that we need to monitor a little more closely.
Thursday, July 22, 2010
The CDC has a brand new blog
And I like it! I especially enjoyed the post by our own Phil Polgreen, which features his iScrub application. Alex Kallen also has a nice recent post on prevention of CLABSI outside the ICU, which is a topic overdue for attention.
However, I did wince when I read about this event:

However, I did wince when I read about this event:
“I believe in zero CLABSIs!” shouted a group of 3,400 APIC Annual Conference attendees at the conclusion of patient-safety leader Dr. Peter Pronovost’s opening session.Why does this make me uncomfortable? It isn’t because I haven’t bought into the power of CLABSI prevention efforts—we have units whose efforts have pushed CLABSI rates to zero for months at a time, and we celebrate that. I also think that most infection preventionists (IPs) understand the difference between a rah-rah, go-get-‘em, “aspirational” BHAG on one hand, and a realistic assessment of what is preventable on the other.
The problem is that many people don’t understand this difference. Among them are fellow healthcare workers, hospital administrators, reporters, the general public, third-party payers, and malpractice attorneys. To them, 3400 infection control experts witnessing to their belief in zero CLABSIs means that every CLABSI must be preventable, and therefore that every CLABSI represents an unconscionable breach of practice. We’ve blogged before about some of the potential unintended consequences of the “zero” paradigm. Fudged definitions, antibiotic overuse, pitched battles between unit personnel and IPs over every device-associated infection, and an atmosphere of blame and punishment, just to name a few.
The fact is that not every CLABSI is preventable. Most are, but not all. Even Peter Pronovost’s hospital's ICUs, though they have wonderfully low rates, still experience CLABSIs. If we follow perfect processes of care, we should be able to prevent those infections that arise from around the catheter insertion site, and those that are introduced exogenously. But what about those arising from gut translocation of bacteria in a critically ill patient? Even the most aggressive gut decontamination regimen (which will inevitably accelerate antimicrobial resistance rates) won’t be able to prevent organisms from gaining access to the catheter in this way.
We should be able to mobilize the troops to drive CLABSI rates to their irreducible minimum without setting unachievable goals. I do admit that “getting to zero” is a catchy phrase, though, and very well-suited to campaigning for lower infection rates. The theme I proposed for our latest CLABSI prevention campaign was roundly rejected….and I still don’t understand what was so wrong with: “Zero Is Great, But One Every Few Months Is Pretty Darn Good, Too”.
Tuesday, July 20, 2010
Good move Maryn McKenna
 We have written often on conflicts of interest. So, I've been following the recent "problems" over at ScienceBlogs.com closely. Quick story is that 2 weeks ago the editors there added a Food Frontiers blog completely funded and written by PepsiCo. I think internist PalMD said it best:
We have written often on conflicts of interest. So, I've been following the recent "problems" over at ScienceBlogs.com closely. Quick story is that 2 weeks ago the editors there added a Food Frontiers blog completely funded and written by PepsiCo. I think internist PalMD said it best:"It could be argued that since it is clearly announced that the content is PepsiCo's, that transparency is maintained, but it's not. Readers of the other 70-odd blogs at Sb expect independent content in the center column. What's more, Sb is indexed by Google News. As a news outlet, we should be held to a high standard. If the SEED management can't see what's wrong with this, this may be an insoluble problem."
PalMD left and returned to his old site as did Maryn McKenna. Many other great bloggers have left too. It must have been a difficult decision to leave the collective, but it is a good one.
PalMD's White Coat Underground (link) and PalMD's full comments (here)
McKenna's Superbug blog (link)
The Guardian's take (here)
Our COI posts (here)
MRSA: Resistance isn't futile?
 "I am Locutus of Borg. Resistance is futile." - Locutus of Borg
"I am Locutus of Borg. Resistance is futile." - Locutus of BorgAny science blog must eventually quote from Star Trek. Now that we've gotten that over with, you can relax. Seriously, relax. Seriously.
The Borg, like MRSA, exhibit a rapid adaptability to any situation or threat. They are perhaps the most menacing cybernetic organisms ever imagined, with all due respect to the Daleks, etc. So you can see why, when I think of MRSA, I often think of the Borg. MRSA is menacing and surely resistance to MRSA is futile. MRSA will rise forever, out of control. Well, not so fast.
A new report out in Diagnostic Microbiology and Infectious Disease by Jose Bordon, et al. report trends in MRSA counts and proportion that are resistant to non-B-lactam antibiotics during the period 1996 through 2008. The analysis included over 2 million S. aureus isolates and almost 1 million MRSA. Their main findings are (1) MRSA increased in Borg-like fashion until 2004 and (2) resistance to all tested antibiotics, except erythromycin, decreased signficantly during the 12-year period. Resistance to ciprofloxacin, clindamycin, gentamicin, tetracycline, and trim-sulfa decreased measurably. The authors claim this could be due to increasing CA-MRSA as proportion of all MRSA. I'm not sure that could explain all of the declines or that it should alter empiric therapy, as suggested by the authors. Overall, the findings seem encouraging.
DMID article by Bordon (link)
Wikipedia article on the Borg (link)
Monday, July 19, 2010
Paul Ewald (video): Are there lessons here for controlling MDROs?
Sometimes, pathogens don't need host mobility for transmission. In these situations, natural selection favors more "virulent" pathogens. That is the general theme of this TED talk given by evolutionary biologist Paul Ewald. I have always been fascinated by this idea in that spread of hospital pathogens does not require host mobility. Could there be other aspects of his theories that could be exploited for infection prevention (or by the pathogen)? Would increased compliance with hand hygiene eventually select for less virulent pathogens. Food for thought. If you are interested in reading more, I recommend his book Evolution of Infectious Diseases.
Click for TED video including iPad/iPhone (non-flash) version: link
Click for TED video including iPad/iPhone (non-flash) version: link
Thursday, July 15, 2010
Confirmation Bias and Science as a Contact Sport
 Just getting back from APIC - New Orleans. I've included this photo from Cafe Du Monde, where I broke "bread" with Titus Daniels, Tom Talbot and Keith Kaye. Thought I should avoid photos of people ingesting the beignets, especially those three guys.
Just getting back from APIC - New Orleans. I've included this photo from Cafe Du Monde, where I broke "bread" with Titus Daniels, Tom Talbot and Keith Kaye. Thought I should avoid photos of people ingesting the beignets, especially those three guys.While trapped in the Detroit airport (a freak storm flooded the gates and shut down the airport for a couple hours), I came across an interesting article in Ars Technica; a site normally associated with reviews of iPhones and Windows 7. The author Chris Lee discusses confirmation bias, a tendency for people to only look for data that confirms their prior beliefs, which permeates all of science and pseudo-science. He provides a number of nice historical examples of confirmation bias. I particularly enjoyed the end of the article where he describes what steps scientists can take to avoid confirmation bias including subjecting their work to as much internal and external criticism as possible. The "denier" section was good too. Can any of you think of examples of confirmation bias in infection prevention? Me neither.
Ars Technica article: (link)
Wednesday, July 14, 2010
Vanity plate of the day (or maybe the year)!
I was leaving the hospital this evening, daydreaming after a clinic filled with difficult cases, when a car leaving the employee parking deck suddenly caught my eye. The license plate read: H8 JCAHO. I kid you not. I quickly looked to see if I knew the driver, but the face was not familiar. I don't know who she was, but she must have a very big ax to grind. If I can find that car, I'll take a photo and post.

Addendum (7/15/10, 7:20 AM):
My colleague, Mike Stevens, had already photographed the plate, and sent me a copy.

Addendum (7/15/10, 7:20 AM):
My colleague, Mike Stevens, had already photographed the plate, and sent me a copy.
Tuesday, July 13, 2010
Pronovost on accountability
Peter Pronovost has a commentary in JAMA this week that is worth a read. Check out the whole thing, I'll post only one small paragraph here:
So who is accountable for reducing CLABSIs? Clinicians inserting and maintaining catheters must be accountable for performance, complying with evidence-based practices. Hospital leaders must be accountable for infection rates, monitoring rates, and supporting prevention initiatives. These mechanisms must be supplemented with the public reporting of valid infection rates, financial incentives from insurers, and when needed, sanctions from regulators. This pandemic of infections can be remedied and prevention of other types of preventable harm can be attempted if clinicians—physicians and nurses—work as a team.My only comment: public reporting of valid infection rates...is much easier said than done, as we've discussed at length in prior blog posts. Meanwhile, the overzealous pursuit of zero perpetuates the daily battles being waged in some centers between infection preventionists (who are "calling" CLABSIs) and ICU clinicians and administrators (who are challenging these calls).
Monday, July 12, 2010
Being Deb Yokoe - Atul Gawande's APIC keynote
I just sat through Atul Gawande's APIC keynote speech. I was expecting to be inspired and amazed. What I wasn't expecting was Deb Yokoe. Dr Gawande spent the first 30 minutes pacing the stage and discussing the day he followed Dr. Yokoe and her team around the Brigham. He described her as a smiling, occasionally giggling with dimples and tennis shoe wearing hospital epidemiologist. It must have been a very busy day as I think he mentioned 7-8 outbreaks she was dealing with at the time including tularemia and a frozen strawberry foodborne outbreak. Having worked with Dr Yokoe as a fellow in a research capacity, I have always appreciated her work and felt she never got enough credit for her contributions. It is very nice to see that changing.
A particularly touching part of the hospital tour with Dr Yokoe was when Gawande described the staff flowing in and out of the ICU rooms and realizing that this was far different than the controlled OR environment and then he realized one of the MRSA isolated patients was his own and that he might have given MRSA to the patient. He got his biggest applause when he quoted Deb as saying "I don't want to be an infection control cop.". Gawande agreed with her and spent some time discussing the importance of team work and getting infection control out of the police business. Well, he has every right to be hopeful. An important effort made at the Brigham that others should consider copying is that infection control is now a rotation for medical students. I suspect it isn't mandatory, but it is a start.
My favorite part of the talk, apart from his discussions of the surgical checklists that were highlighted in his latest book, was when he was asked a question about mandates. He described that in any advance there are early adopters, medium adopters and late adopters. He then added in a class of people called exceptionalists, people who say they are different or their hospitals are too different to do things like clabsi checklists. His point was that there is a time when mandates are needed but the key variable is the timing. One must wait to mandate until after the early adopters are on board and worked out all of the implementation details. Any mandate that comes too early, alienates these early adopters and hurts implementation. Food for thought.
A particularly touching part of the hospital tour with Dr Yokoe was when Gawande described the staff flowing in and out of the ICU rooms and realizing that this was far different than the controlled OR environment and then he realized one of the MRSA isolated patients was his own and that he might have given MRSA to the patient. He got his biggest applause when he quoted Deb as saying "I don't want to be an infection control cop.". Gawande agreed with her and spent some time discussing the importance of team work and getting infection control out of the police business. Well, he has every right to be hopeful. An important effort made at the Brigham that others should consider copying is that infection control is now a rotation for medical students. I suspect it isn't mandatory, but it is a start.
My favorite part of the talk, apart from his discussions of the surgical checklists that were highlighted in his latest book, was when he was asked a question about mandates. He described that in any advance there are early adopters, medium adopters and late adopters. He then added in a class of people called exceptionalists, people who say they are different or their hospitals are too different to do things like clabsi checklists. His point was that there is a time when mandates are needed but the key variable is the timing. One must wait to mandate until after the early adopters are on board and worked out all of the implementation details. Any mandate that comes too early, alienates these early adopters and hurts implementation. Food for thought.
Adverse effects of contact precautions
There's a new systematic review on the adverse effects of contact precautions in the Journal of Hospital Infection. This paper's methods and findings are very similar to Dan Morgan's paper (with Dan Diekema, Kent Sepkowitz and Eli Perencevich as co-authors) from last year. There are a few papers that are not found in both reviews, but no newer papers are covered in the new review. The conclusions of the two papers are largely the same: contact precautions are overall associated with adverse unintended consequences for patients in the observational studies that have been published.
Saturday, July 10, 2010
James Bagian on medical error
Kathryn Schulz has a wonderful Q&A with James Bagian, director of the VA national center for patient safety, at the Slate blog "The Wrong Stuff". Read it all, but I especially enjoyed his thoughts on blame, punishment, and the perverse incentives that can be introduced by public disclosure.
Kathryn Schulz is the author of the book, Being Wrong: Adventures in the Margin of Error. I haven't read it, but I think I'll check it out.
Thursday, July 8, 2010
Gloves and gowns are not enough...

Back at Maryland, we had a surgeon who always asked for evidence that hand hygiene was necessary if he wears gloves. We gave him some evidence, but like many clinicians, he wanted data from his own institution. I guess everyone is the exception. Like good soldiers, we proceeded to collect that data. We gathered a great team over the years - Graham Snyder, Stephen Liang, Catherine Smith, Hannah Day and others to approach healthcare workers (HCW) before they entered patient rooms and collect cultures on their hands before entry and gowns/gloves after exiting the room.
The initial study from this work was published by Graham Snyder et al in ICHE 2008. He reported that MRSA was detectable on 19% of gowns/gloves of HCW after exiting an MRSA+ patients room, while that result for VRE was 9%.
The latest report from this group published in this month's ICHE by Dan Morgan et al, provides somewhat more humbling data. HCW had MDR-acinetobacter on their gloves 36% of the time after entering a colonized/infected patient's room. Wow. But the truly humbling finding was that after removing their gloves, 4.5% of the HCW still had it on their hands. Thus, while gloves reduce contamination of hands by around 85% per contact, to achieve true infection prevention, HCW must wash their hands after they remove there gloves.
I have posted Table 2 from the paper, which shows the likelihood of HCW contamination that would occur at various levels of compliance with contact precautions and hand hygiene. Even with 90% compliance with both wearing gloves and hand hygiene, almost 1% (0.8%) of contacts would be expected to contaminate the HCW hand and place them at risk for contaminating other patients and the environment. Multiply that 1% (or higher if lower compliance exists) by the number of HCW that enter the patients room in a day and you have an estimate of the daily transmission of MDR-AB. This sort of data highlights the Achilles heal of active detection and isolation strategies. No matter how much effort and money go into rapid detection of MDR organisms, without 100% compliance to gowns and hand hygiene, the effort is wasted. We have shared this data with our favorite surgeon. The description of how that went must wait for another study, or at least another day.
Graham Snyder 2008 ICHE paper (here)
Dan Morgan July 2010 ICHE paper (here)
Wednesday, July 7, 2010
Opting-in vs. opting out
In this week's JAMA, there's a research letter evaluating two strategies for achieving healthcare worker compliance with influenza vaccination. HCWs (n=480) were randomized to an "opt-in" group or an "opt-out" group. In the opt-in strategy the HCWs received an email with a link to a website where they could schedule their vaccinations. In the opt-out strategy, the HCWs were sent an email with a scheduled appointment for vaccination. Compliance with vaccination was 33% in the opt-in group versus 45% in the opt-out group (P=.008). The authors conclude that automatic scheduling of vaccination may be an effective method for increasing compliance with influenza vaccination. While that may be true, what is striking to me is the abysmal compliance rates in both groups. We are aware of hospitals that are achieving >90% compliance without mandating vaccination, but by actively promoting vaccination and providing incentives. At my hospital, we recently decided that for the upcoming season we would not mandate vaccination, but more aggressively promote vaccination, make vaccination even more convenient, and aggressively promote the message that ill healthcare workers should stay at home. Like handwashing, keeping ill HCWs at home is a multipotent intervention that will not only reduce the potential for spread of influenza but for other respiratory pathogens as well.
Tuesday, July 6, 2010
Hospitals turning green
Today's New York Times has an article on the movement by many hospitals to reduce medical waste. The article largely focuses on the operating room where many unused items are commonly discarded. But it made me wonder how much contact precautions, with all the use of disposable gowns and gloves, adds to the problem.
Monday, July 5, 2010
The parasite-stress hypothesis
I ran across an interesting article in this week's Economist, which covers a new paper in the Proceedings of the Royal Society of Biology--an ecologic study that correlates countries' population burden of infectious diseases to levels of intelligence. The authors of the paper conclude that countries with the the highest rates of infectious diseases have the lowest IQs, even when controlling for confounders such as GDP, education, and climate. The investigators hypothesize that the energy consumed by infections in early childhood affect brain development, leading to lower intelligence. The paper is intriguing, the association seems biologically plausible, and the authors seem careful to identify potential confounders and caution the reader on the limits of observational studies.
Sunday, July 4, 2010
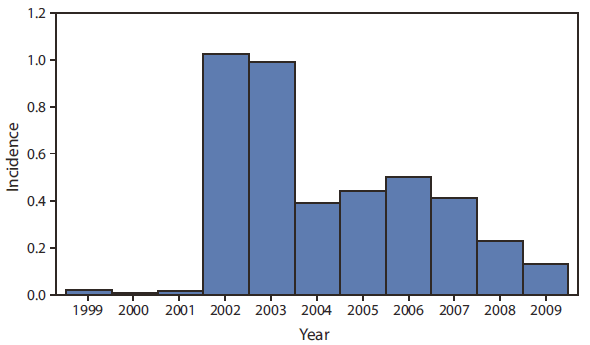
Bye Bye West Nile Virus???
Friday, July 2, 2010
Heads, MRSA. Tails, possibly MRSA.
Cepheid just issued a recall notice on the Xpert MRSA/SA BC test, the rapid, real-time assay that is designed to quickly identify MRSA vs. MSSA in positive blood cultures. Seems MRSA can evolve (!), and there are now some isolates that are not detected, resulting in false-negative results (that's what us clin micro types call a "very major error"). Here is the text of the notification:
Dear Valued Customer:
Based on the recall announced July 1, 2010, Cepheid is initiating a recall of all lots of Xpert MRSA/SA BC (blood culture) product. The recall is a corrective action, which does not require return of product to the manufacturer. Customers may continue to use the product; however, when a MRSA negative/SA positive result is obtained, the results should be interpreted as MRSA indeterminate/Staphylococcus aureus positive, antimicrobial susceptibility testing pending. Further testing should be performed using an FDA-cleared, phenotypic antimicrobial susceptibility testing method on isolated colonies recovered from the blood culture bottle. MRSA positive/SA positive results can still be reported as such. The new instructions will be incorporated in the product labeling. The Xpert MRSA/SA BC product produces false-negative MRSA results, which could potentially contribute to incorrect treatment of an MRSA infection.
The following statement will be added to the Interpretation of Results section of the package insert for "MRSA Negative/SA Positive" results:
The results should be interpreted as "MRSA indeterminate/SA Positive, antimicrobial susceptibility testing pending". Further testing should be performed using a FDA-cleared, phenotypic antimicrobial susceptibility testing method on isolated colonies recovered from the blood culture bottle.
Although the product appears to continue to meet performance claims as outlined in the current product labeling, an ongoing failure investigation has identified the emergence of novel MRSA strain types as one of the causes of false-negative MRSA results. The failure investigation has not fully determined the remaining causes of the false-negative MRSA results. To date, one adverse event has been reported to the FDA through the MDR process.
Thursday, July 1, 2010
XMRV and Chronic Fatigue Syndrome: Is there a link?
Several months ago a paper in Science linked Chronic Fatigue Syndrome to the xenotropic murine leukemia virus-related virus (XMRV). Now a new study in Retrovirology by investigators at CDC refutes the Science paper. In the new study blood samples from 51 patients who met the CDC diagnostic criteria for CFS and 56 healthy control patients were tested via western blot, ELISA, and 2 different PCR assays for XMRV. None of the patients in either group were found to be positive by any of the methods. However, according to the Wall Street Journal there's yet another paper from investigators at the FDA and NIH, as of yet unpublished, that claims a link between XMRV and CFS. I don't know what to think except that this virus needs a new name--virus-related virus sounds dumb to me.
Another state HAI report
For those of you interested in public reporting of healthcare associated infections, Oregon has just published its first report on HAIs. You can view it here.
Subscribe to:
Posts (Atom)
OSHA! OSHA! OSHA!
In many parts of the country, as rates of COVID-19 are declining and vaccination coverage is increasing (albeit with substantial variati...

-
This is a guest post by Jorge Salinas, MD, Hospital Epidemiologist at the University of Iowa Hospitals & Clinics. There is virtually no...
-
I’m surprised that we can’t stop arguing about the modes of SARS-CoV-2 transmission, despite the fact that most experts (including our frie...
-
 In many parts of the country, as rates of COVID-19 are declining and vaccination coverage is increasing (albeit with substantial variati...
In many parts of the country, as rates of COVID-19 are declining and vaccination coverage is increasing (albeit with substantial variati...

